
At this point, there have been many studies that have examined the effects of switching patients with schizophrenia from conventional/first-generation antipsychotic medications (FGA) to newer antipsychotic/second-generation antipsychotic meds (SGA).
These studies have usually examined patients whose symptoms were poorly controlled on FGA but improved on SGA.
The results typically indicate some improvement, which is often used as an argument to pimp SGAs.
Taking this argument a step further, a recent study in the Journal of Psychiatric Research examined schizophrenia patients who were stable (not doing extremely poorly, but seemingly not functioning very well either) on their FGA meds. They were switched to olanzapine (Zyprexa) or risperidone (Risperdal), both SGAs, and they showed improvement in their symptoms over a 22-week time period (some of which involved tapering from old to new meds – 12 weeks on treatment with the new medication alone). Ok, great. So switch everyone to SGAs, right?
Some conceptual problems that are not mentioned in this study loom large. To draw any sort of conclusion regarding the effects of medication, a control group is needed, yet there was no control group in this study. For example, the inclusion of a control group that was maintained on their current medication or, better yet, told they were switching medications, but actually received their same FGA medication. One could have witnessed how they progressed in comparison to how the SGA-switch group progressed.
Or, how about a study in which one group was switched from FGA to SGA, and another group was switched from SGA to FGA. Yes, I said it. Why have there been no studies (to my knowledge) that have switched patients from SGA to FGA? I’ll tell you why. Because it is likely that they (SGA to FGA switchers) would show just as much change as those switching from FGA to SGA. SGAs are widely used enough and have existed for long enough that surely there are many people with schizophrenia who have taken SGAs only – that is, they have never taken FGAs. So switch them to FGAs in a study and see what happens. When this study is conducted, I’m prepared to eat humble pie if it does not confirm my predictions. In fact, let’s have three studies conducted independent of drug company funding and see what happens. NIMH, what do you think? In the meantime, all the hoopla about switching from FGA to SGA needs to S-T-O-P. This is easy research to conduct and I’ll be awaiting its results.
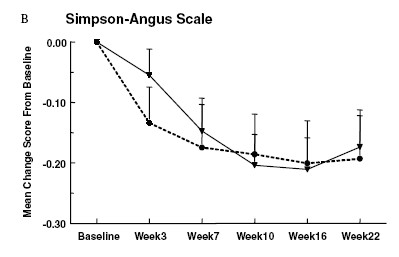
BS Watch: I’d like to mention one further concern with this study. The authors noted that there was a significant decline in Simpson-Angus scores, which assesses extrapyramidal/motor problems commonly associated with antipsychotic treatment. The authors did not report means and standard deviations for the measure, just that F(5, 204) = 4.2, p < .01. From the figure in the article, we can see (look to the top right) that the mean score on this measure dropped by a little less than .20. This mean change of less than .20 occurred on a measure that ranges from 0-40, so I think their figure may well qualify for the next issue of Misleading Charts Quarterly.
Read more about the “amazing” SGAs here, here, and here.
Update: I was likely in error regarding the Simpson-Angus scores. Though the version of the measure I have is scored on a 40 point scale, it is true that some studies use a version that I believe runs from 0-4. In any case, I stand by the graph being misleading without at the very least discussing the effect size associated with the comparisons of EPS scores.
No comments:
Post a Comment